Genu, Kne, Cnēow, kneu
Bonjour! Enjoy the exclusive content on knee in this month's issue
Hot from AO’s Ovens…
Fancy metaphyseal comminution? Thinking about fixing it with a nice, locked bridge plate? Yes, that’s the dream. But what about metaphyseal comminution in a femur? Not so much of a dream. Those failed implants would agree.
Problem no more…
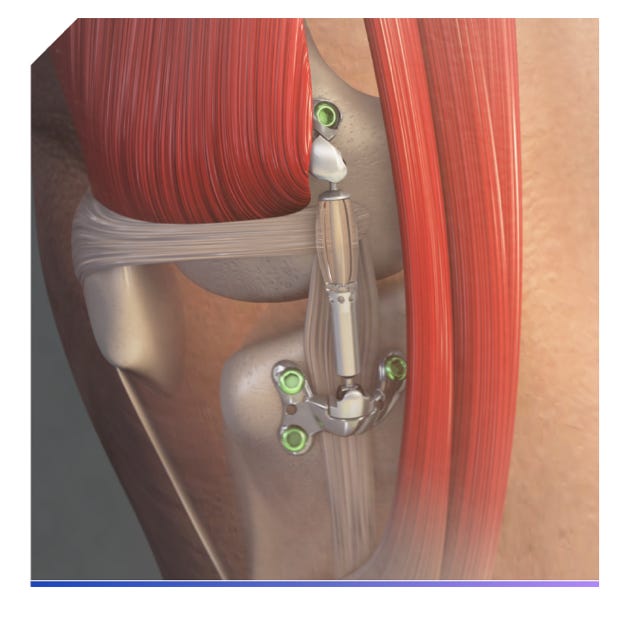
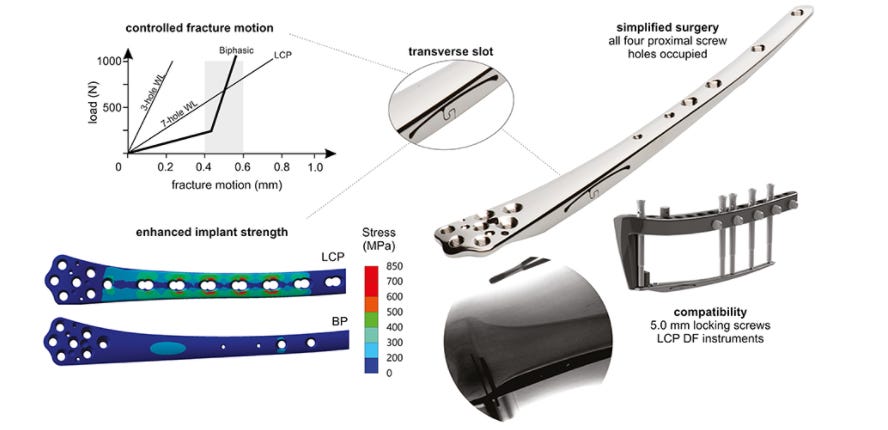
We bring you fresh from AO incubator, - Biphasic plate
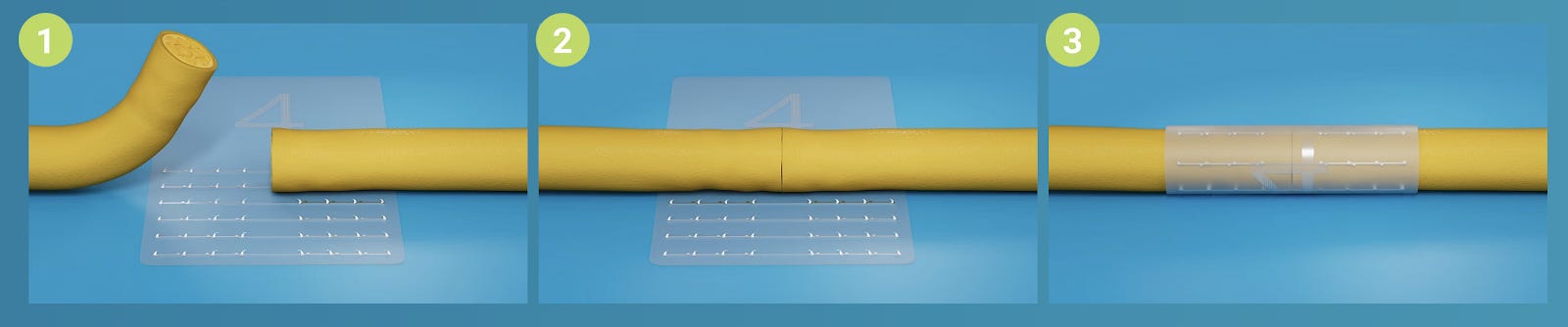
The biphasic plate has a transverse S-shaped slot with increased thickness in the supracondylar region. Increased plate thickness leads to high strength and stiffness at higher loads (rigid phase), decreasing the risk of implant failure. The slot provides flexibility to stimulate callus formation at lower forces associated with partial weight-bearing (flex phase). The concept, hence, intends to confine interfragmentary motion to a desirable range independent of functional loading. The “S” shape of the slot prevents it from twisting and opening and thus ensures the implant resists forces resulting from reverse (valgus) bending and torsion of the plate. Currently, in-vitro testing results are out for a Distal femur plate and have been classified as a type IIB medical device. Awaiting further human trials.
It has a bi-linear response – 55% more complaint at low loads and 476% stiffer at higher loads than the conventional DF-LCP fixed in a similar construct. This allows to ‘pre-program’ the strain at the fracture site - Controlled strain within the desired range even with partial or full weight-bearing.
While we only have a distal femur plate for now, with a limited use case, it seems not difficult to adopt the idea to other load-bearing implants. Watch this space for further updates.
Tokyo to Toronto: The silk route of Arthroscopy
Prof. Watanabe of Tokyo, referred to as the father of modern arthroscopy was relatively unknown when Prof Robert Jackson of Toronto, visited Tokyo with the Canadian Olympic Team in 1964. Dr. Jackson had to find the practice area of Prof Watanabe from one of the rotating residents. Dr. Jackson had his first meeting with Prof Watanabe with a skeptical mindset. However, arthroscopy transcended international borders after that meeting.
Severin Nordentoft, Kenji Takagi, and Eugen Bircher were all pioneers of arthro-endoscopy making scope a feasible option for viewing joints. However, it is Prof. Watanabe, a student of Prof. Takagi, who fine-tuned the art and made it available to the world in a palatable manner.
After World War II, Watanabe started working in the Tokyo Teishin (Postal Services Ministry) Hospital. He started improvising the models of arthroscopes available. In 1955, he arthroscopically removed a xanthomatous giant cell tumor from the suprapatellar pouch and recorded it. This footage is widely considered as the first recorded arthroscopy on a patient. In 1958, Watanabe produced the No. 21 arthroscopes. The No. 21 design became the world’s first production model and the last version with an incandescent light source.
A timeline of milestones in the development of the subspecialty of Arthroscopy is as follows
1957 - Watanabe and colleagues publish “The Atlas of Arthroscopy.”
1959 -Watanabe No. 21 becomes a production model.
1962 - Watanabe performs the first arthroscopic partial meniscectomy.
1964 - Robert Jackson learns knee arthroscopy from Watanabe.
1965 - Jackson brings knee arthroscopy to North America at the Toronto General Hospital using Watanabe No. 21 arthroscopes.
1968 - Jackson and Isao Abe present an instructional lecture on knee arthroscopy at the American Academy of Orthopaedic Surgeons annual meeting.
How knee arthroscopy flourished in the west after these events is history.
Dr. Jackson and his friends with Prof Watanabe????

Gut-Joint Axis! A newer perspective into OA pathogenesis:
Inflammation remains the core mechanism for a lot of diseases. Inflammation in OA is proposed to be due to gut dysbiosis due to perturbation of biodiversity in the gut microbiome. This Gut-Joint Axis provides a distinct perspective in managing OA. The hypothesis is that the microbial community shifts induced by antibiotics, a germ-free environment, or high-fat might have a key role in the development of OA. Thus, active microbiome modulation could be an effective therapeutic option for OA
Dietary supplements and nutraceuticals seem to exert their positive effects on health status in the elderly through quantitative and qualitative modifications of the gut microbiome.

Oldies! Should we strengthen our extensors?
Oiestad et al. conducted a meta-analysis to analyze the association between knee extensor muscle weakness and the risk of developing knee OA. Five cohort studies with a follow-up time between 2.5 and 14 years and of 5707 participants were analyzed.
People with extensor muscle weakness had 1.65 times more risk of developing knee osteoarthritis. However, it remains to be proven if knee extensor muscle strengthening can reduce the onset or progression of knee osteoarthritis.

Surgical Pearl
Anterior Closing Wedge Osteotomy - correct the slope in failed ACLRs!
Most of the time, the reason for failure in ACLR is increased posterior slope. Below is a simple surgical technique to correct the slope by DePhillipo et al

Find the video here
Major events not to be missed:
The answer to the last issue Query is here
What is the ideal time to wait in post-infection staged revision total joint arthroplasty?
Though there is no consensus on the timing globally, the proper timing of re-implantation should be combined with the disappearance of clinical symptoms and negative intraoperative Frozen Section with a spacer detention time at 12 to 16 weeks. ESR and CRP are poor indicators of infection at the time of re-implantation