A white collared job!
Enjoy reading on the part of Orthopaedics that is white collared.
Work from home? #NeoArmory:
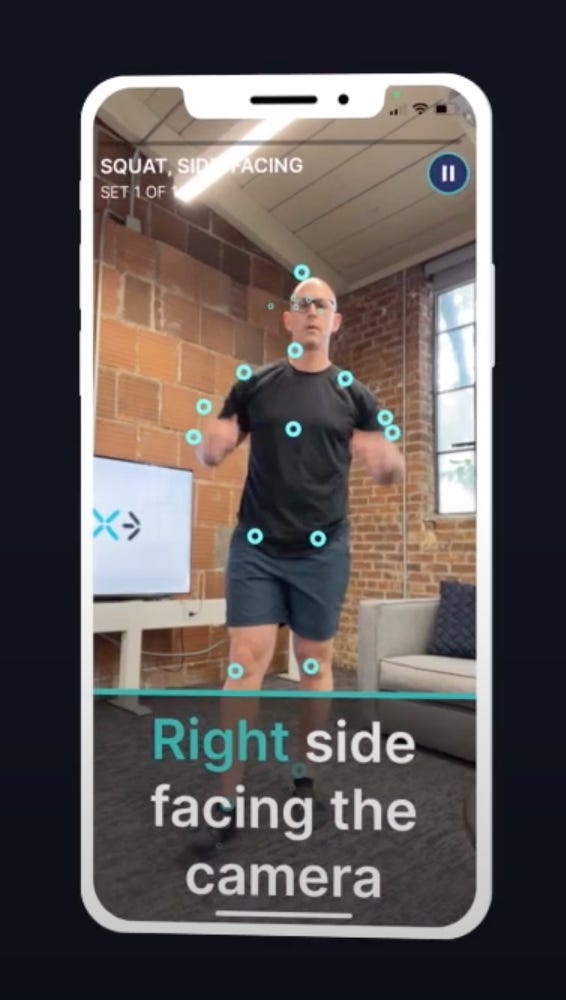
Telehealth is medicine’s equivalance of work from home and the pandemic has accelerated the trend. Out of the core concepts of examination, inspection can be done by camera but move and measure haven’t been reliable. EXER.AI is here with an answer.
This system lets you precisely monitor the range of movements and thereby aid in progression of physio. This is done without any additional kits like sensors or special cameras. The patients use their mobile phone camera and the intuitive AI (yep, the one in the name) can currently track 24+ body points and 100+ exercises.
They offer remote support and this part helps us monitor progress.
“That TKR post-op is progressing as expected, you don’t need to bring the patient to the clinic every week now”
Just pull up the chart and let AI show you this week’s or today’s ROM. You can use these softwares to document the range during every visit.
Of course, when we talk about cameras and patients in the same sentence, words like privacy and regulations on data storage usually follow. If they can do this part right, forward is the only way.
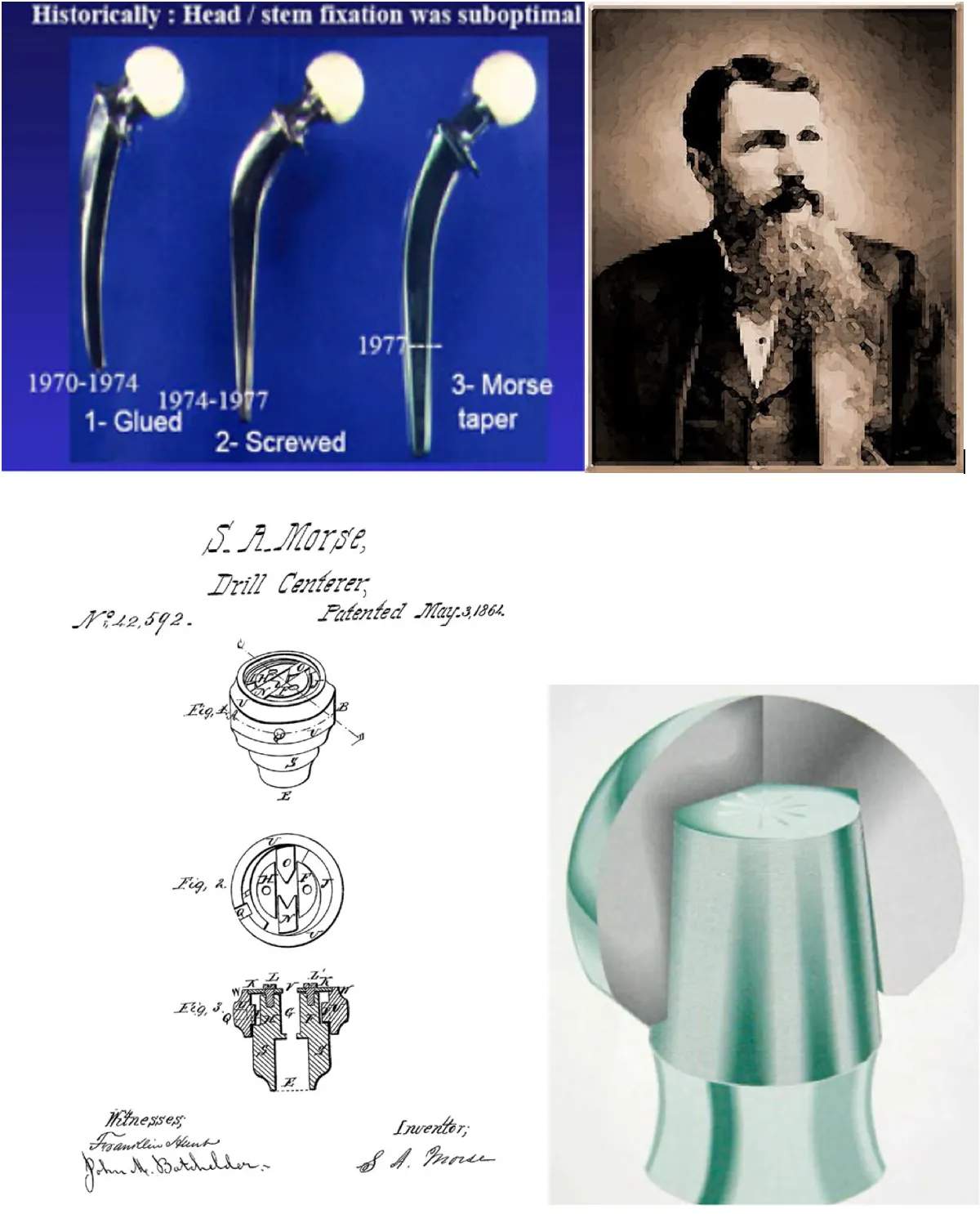
The reason behind review clinics - #FromTheHistory:
Nowadays. the most important thing that we, as surgeons love to do in OPDs is to follow up on our post-op cases. But do you guys know the exciting story behind follow-ups?
In times, when no one even thought of the words “follow up”, there was someone who conceptualized and implemented it against popular opinion. He did not mind facing criticism or even resigning from his job to stand by his noble idea. It will be an understatement to say that his persistence changed the way medicine is being practiced.
Ernest. A. Codman, a Harvard-educated surgeon at the Massachusetts General Hospital came up with the “End Result Idea”. The idea was to create a system where the hospital would follow up every patient and note down the end results. This would in turn help surgeons to improve the treatment quality. He wanted the results of the End Results System to be made public so that patients could choose good doctors. In the early 1900s, one should say, Dr. Codman’s IDEA was far ahead of time. It was met with controversy and criticism. When MGH did not like his system, he resigned from his job to start a private hospital where he would implement these practices. He published the results of the End Result System of his hospital admitting 123 errors in 337 patients treated.
He was persistent with his ideas and convinced Edward Martin, the then President of the clinical congress of North America to form the committee for hospital standardization. He started the hospital standardization movement which led to the formation of the American College of Surgeons and the Joint Commission on Accreditation of Hospitals. In short, his ideas raised the standard of care for millions of patients.
Codman had a great interest in treating shoulder pathologies and bone sarcomas. He authored “The Shoulder”, one of the classic textbooks on the shoulder. He was instrumental in starting the first registry for bone sarcoma in 1920. One will never forget the Codman triangle of Osteosarcoma, Codman’s exercises, Codman’s tumor, Codman’s bursa, Codman’s paradox, and Codman’s sign

Simple solution for chronic, recalcitrant coccygodynia: #SurgicalPearl:
Simply put, the answer is the Ganglion impar block, which is block of the terminal end of the pelvic sympathetic chain.
· Patient is positioned prone with a pillow under the pelvis. The point of maximum identified and marked. Local area is prepped in a sterile manner and skin infiltrated with local anesthetic agent (LAA; 2% lignocaine).
· Under fluoroscopic guidance, the antero-posterior (AP) view of the coccyx is obtained to identify the midline.
· A 22-gauge Quincke spinal needle was then introduced until it hit the bone.
· At this stage, lateral fluoroscopic view is obtained in order to locate the sacro-coccygeal and coccygeal articulations.
· The needle is then gradually inserted through the sacro-coccygeal or 1st intra-coccygeal joints until the retroperitoneal space is reached.
· The needle position is then confirmed with the help of non-ionic contrast dye (0.2ml of Iohexol, Omnipaque).
· Comma sign: The linear contrast spread in the space anterior to coccyx and immediately posterior to rectum is described as the “comma sign”.
· After the needle position is ascertained on fluoroscopic images, 5ml of 0.25% bupivacaine and 40 mg of methyl prednisolone acetate is injected; and the needle is gradually withdrawn.
· A firm pressure is then applied over the injection site to ensure good hemostasis; and a sterile dressing is applied.

Should I poke my patients multiple times? - #HighlyCited:
PRP seems promising in knee Osteoarthritis. But, is one injection sufficient or should we give multiple injections is still a question. Paramanantham et al. compared the single shot PRP in 34 patients to two-doses in 30 patients presenting with KL Grade I/II OA. Significant improvement of pain and functional limitation measured by VAS and WOMAC in both groups at pre-injection, sixth week, third month, and sixth month were noted.
Multiple PRP injections have a significant pain reduction when compared to single-shot PRP at longer follow-ups. However, no statistically significant difference was noted in WOMAC improvement. A recent trial even recommends 3 injections over a single shot.

Is lidocaine really needed? #InTrials:
In Subacromial impingement syndrome, a high-volume corticosteroid injection (Steroid + lidocaine mixture) - HVCI, increases the incidence of local and general complications from lidocaine. Adinun et al aimed to compare the results of functional and clinical outcomes between the very low-volume corticosteroid injection without lidocaine - VLVCI and HVCI. 64 patients were included in a randomization-controlled trial. The VAS for pain pre-injection and post-injection at 15 min did not show any significant differences. At all follow-up timing, there were no significant differences in WORC, DASH, and ROM between two groups (P > 0.05). The results revealed that VLVCI is non-inferior to HVCI both of functional outcomes and VAS.
After all lidocaine might not be needed!

Question of the month:
What is most effective route of selective nerve root block in spine?
-
Transforaminal
-
Iliolumbar
-
Caudal
Hold your curiosity till next month for the answer.
Answer for last month’s question:
Pathological Fracture in Osteosarcoma - which of the following is false?
-
Contraindication for limb salvage surgery
-
Associated with the increased rate of metastasis
-
No difference in recurrence rate when compared to those without pathological fracture
-
Decreased 3-year and 5-year survival rate
Option 1 is false. Rest are true #LimbSalvage
Events to check out:
-
Singapore Orthopaedic Association Annual Scientific Meeting 2023 23-25 November 2023: Singapore
-
BOTA Annual Congress Nov 28- Dec 1, 2023: Edinburgh, United Kingdom
-
AAOS 2024 12 - 16 February 2024: San Francisco, USA
Have a fabulous fall guys. Cya all next month.