John plated coronoid 'n extension
And Hemiarthroplasties in wrist and elbow!
All that Hemiarthroplast-ies are not at the hip…
We always have an implant for everything. But one of the difficulties we face is holding the implant in place in a porotic bone. Especially in distal radius fractures which is the most common upper limb fracture, when the bone is porotic holding the implant in place is a struggle. Be it an LCP or a wire.
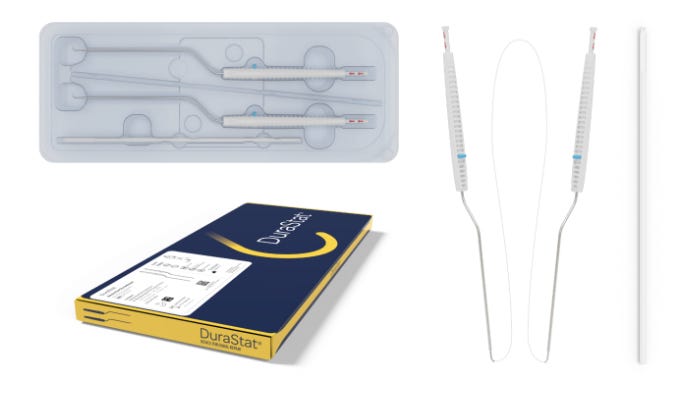
We end up immobilising it longer than usual where Early mobilisation is key. Prosthelast TM might have an answer at least in specific use cases. It is a Distal radius Hemiarthroplasty prosthesis indicated for comminuted injuries where osteosynthesis was not deemed to be a good option.
Prosthelast also has a carpal component which gives a metal on poly articular surfaces. This Implant is claimed to be built on the learning points of the previous failed ones. The centromedullary wire helps in redistributing the forces along the Radius.
In an interesting case study, it was used following resection of malignant tumour distal radius. Mind that longer term studies and RCTs will be needed to properly evaluate this implant but it’s good to have as a part of our metal inventory.

The tale of Tommy John and Frank Jobe.
Most Baseball enthusiasts of 1970s should be fans of Thomas Edward John aka Tommy John - A four time MLB All-Star athlete. Though some may not be fans of his play, all are inspired by his comeback.
Getting his professional baseball contract at the age of 18, Tommy John suffered a career ending ulnar collateral ligament injury at 31, when he was at the prime of his form. In those days UCL injury was considered too grave to return to sport again. It was called the dead arm.
Even when life gave upon Tommy John, Dr Frank James Jobe had other plans. In 1974, he reconstructed the UCL with Palmaris longus tendon and meticulously rehabilitated Tommy John for one year. Later Tommy John returned to baseball and played for the next 14 years without any problem to his elbow. The success of Tommy John was so highly spoken that the surgery of UCL reconstruction is till now commonly called the Tommy John Surgery. An estimate in 2012 showed that about 14 percent of baseball pitchers had undergone Tommy John Procedure.
For his outstanding contribution to the field of baseball Dr Jobe was inducted into the Baseball Hall of Fame - a significant recognition given that he has not played a single innings of baseball. Dr Jobe dedicated his entire life to sports medicine being associated as team physician with various teams till his death and mentoring young Orthopaedicians. He had 3 doctorates and contributed Jobe’s exercises for shoulder and many other innovative procedures. He is rightly called one of the premier fathers of modern sports medicine.

Plating coronoid: Technical Pearl:
-
Supine position
-
Smaller fractures - “over the top” approach in flexor-pronator interval.
-
Larger coronoid fractures - posteriorly with elevation of flexor-pronator mass.
-
Antebrachial cutaneous nerve - identified and avoided
-
Ulnar nerve was identified, decompressed, and protected
-
Preliminary reduction with K-wires
-
Definitive fixation with a 1.5 mm or 2.0 mm T-plate as a buttress plate and augmented with headless compression screws if the fracture pattern allowed.
-
Flexor-pronator mass - repaired using sutures (if flexor-pronator mass is split) or suture anchors (if it is elevated)
Read it fully here

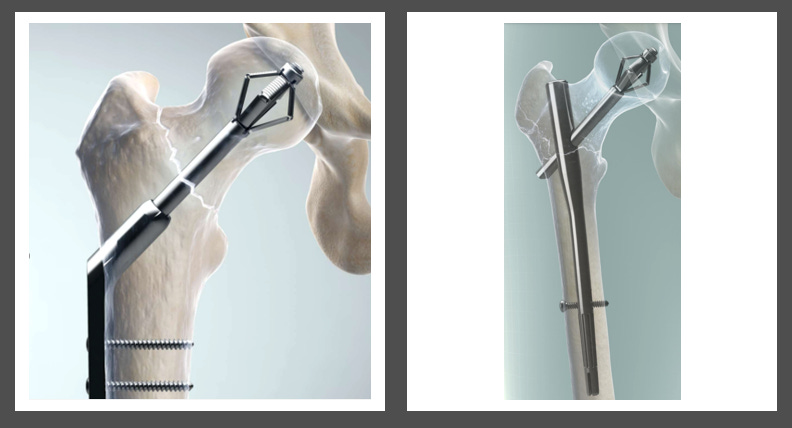
Parallel vs 90-90
There has been a long-standing debate on the ideal fixation construct for intra-articular distal humerus fracture fixation. Apart from the clinical results of various studies, Kruszewski et al. comparatively analyze the stabilization conditions of intraarticular fractures of distal humerus with the use of various configurations of the stabilizing plates by finite element analysis. The research was based on the analysis of mutual displacements of bone fragments. Three spatial configurations of the plates such as parallel, posteromedial and posterolateral were considered. The mutual displacements of bone fragments as well as the deformity of the stabilizer under various loading conditions were analyzed. The parallel setting of the plates ensures a better stabilization of the bone fragments than the perpendicular configuration.
Parallel it is……

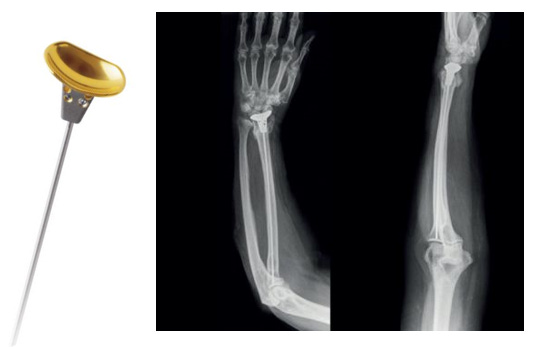
Extension casting for Forearm fractures in Children?
To challenge the traditional management of paediatric forearm fractures with above elbow plaster casting with elbow flexed to 90 degrees, Yadav et al. conducted a prospective study to evaluate the functional and radiological outcomes of extension casting for paediatric forearm fractures. 83.3% of extension cast status were intact at 2 weeks and 16.7% has loosened and needed reinforcement. Post removal patient had good ROM at 3,6 weeks. They concluded that casting with extended elbow is much better as compared to flexion casting in the hands of a trainee doctor. Chances of loss of reduction are negligible in extension casting as compared to flexion casting.
Keep them extended…

Check these cool events lining up
Answer to the last month Question
Which injection treatment method do you think works the best in Tennis Elbow?
-
Steroid Injection
-
Local Anesthetic Injection
-
PRP Injection
-
Autologous Blood Injection
-
Hyaluronic acid Injection
-
Saline Injection
PRP it is - according to Muthu et al.’s network meta-analysis
Question of the Month?
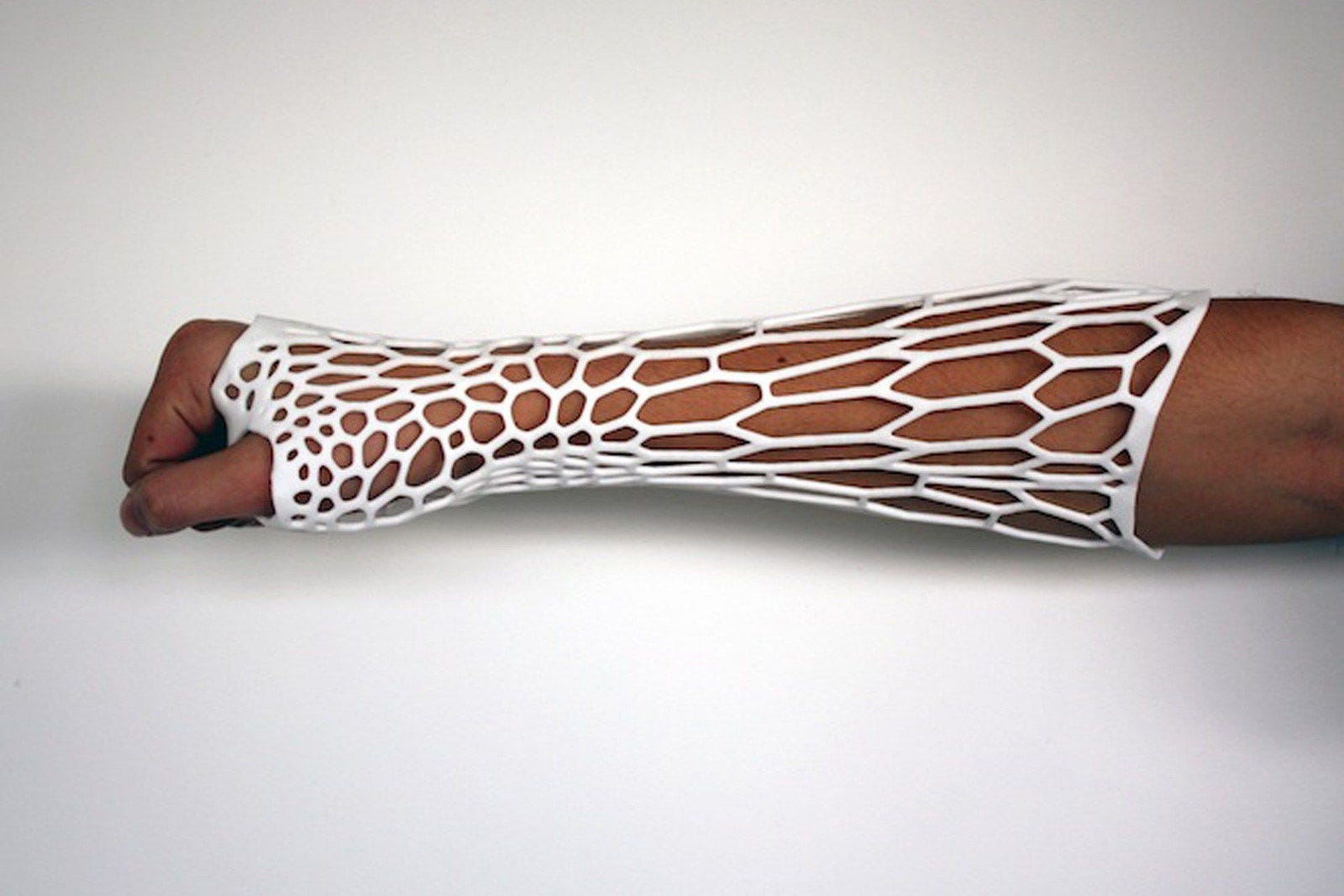
Which of the following BE slabs used for hand injuries would the most economical and stable construct with maximum stability?

-
Right – Standard single thickness (3 mm)
-
Left – Standard double thickness (6 mm)
-
Middle – Standard single thickness (3 mm) with two triangular reinforced ridges.
Wait for our June Issue for the answer…
Macho May guys :)