Towards the elbow, we go
Enjoy this exclusive issue on Elbow & wrist, brewing with bones

Will AO nail it? - #NeoArmory:
Intramedullary nailing is the closest analog to ‘keyhole surgery’ in trauma. It is biomechanically stronger in most cases (I know; controversial). This led to a subset of orthopods wanting to nail anything that moves.
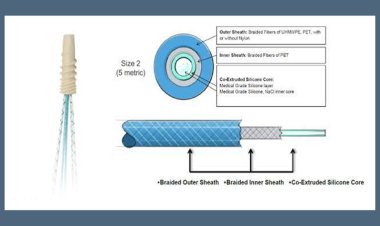
Nailing distal radius fractures have been either controversial or ridden with complications. But, as with any technology, things improve with time; or do they? Let’s find out. AO Development incubator along with Swiss Surgeons have come up with DRIM-NAIL (Please change the name. Please) - The idea being able to minimize soft tissue complications.
The nail comes as a universal size, sterile pack - 7.0mm diameter titanium implant with 2.5mm screws for fixation made of stainless screws. The target population seems to be Extraarticular fractures.

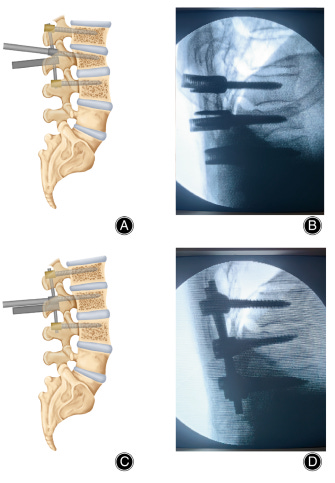
This systematic review concludes although the IM nails are biomechanically as strong as the Volar locking plate, there is about a 9% chance of Dorsal branch radial nerve neuropraxia. But this group suggests that the complications are not statistically significant. A more exciting paper proposes that IM nails can be used for extraarticular osteotomies in the distal radius.
When Engineering and Medicine came together… - #FromTheHistory:
Medical and engineering faculties work together to bring out good instruments and implants. What if one can master both these subjects? His understanding will be profound and his vantage point will be different. The outcomes can be benchmarks in the field. Prof Bernard. F. Morrey is one such example.
After his Bachelor of science in engineering, he worked at NASA for two years. Later, his passion for both medicine and engineering made Dr. Morrey complete his Orthopaedic residency and Master of Biomechanics. This unique combination of training must have influenced his clinical and research career. His contributions have revolutionized the orthopedic practice, particularly the management of elbow disorders.
Ideation and development of the first radial head replacement, Morrey total elbow prosthesis, Morrey elbow score, and Morrey classifications are some of his notable contributions. His research has changed the understanding of elbow biomechanics. He had a total of 9 patents and had authored more than 12 textbooks and 400 plus research articles. He was the personal Orthopaedic surgeon of President Bush. He was also an accomplished artist and collector, said to have possessed a collection of more than 1000 medical books.

Arthroscopic Radioscapholunate fusion - #SurgicalPearl:
-
Under finger trap traction, through 3-4 and 6R portals diagnostic arthroscopy is performed, and synovectomy is done.
-
Corresponding articular cartilage is removed to expose the subchondral bone using curette and burr until a bloody dew sign appears.
-
Iliac crest bone graft is fragmented to be introduced into the radiocarpal level under arthroscopic control using a 20-gauge needle trocar caps - beveled and then manually filled and introduced by the 3-4 and 6R portals alternately.
-
Internal fixation without traction is done by percutaneous dorsal radio lunate and dorsal radio scaphoid 3mm Herbert screws.
-
A minimum number of three screws is required: two in the scaphoid and one in the lunate.

Please find the video demonstration by Bargemon et al here.
Recalcitrant Lateral Epicondylitis - Are there too many dishes to taste on the table?
What is the best treatment option for recalcitrant lateral epicondylitis? Are there too many dishes to taste on the table?
We have a level 1 study from Muthu et al. analyzing the effectiveness of all the interventions and comparing the interventions to saline placebo injections. Only PRP resulted in significant pain relief on VAS outcome compared to saline control while the rest of the interventions did not offer any significant benefit compared to saline control. In functional outcome parameters such as DASH and PRETEE scores, none of the treatment methods analyzed were superior to saline management. In a subgroup analysis of the outcomes at various time points, PRP resulted in clinically significant improvement at all time points analyzed. PRP seems to be the more promising treatment method in recalcitrant lateral epicondylitis.
Just move it ????????
Should we or should we not mobilize after flexor tendon repair? There is no strong scientific evidence suggesting that early active mobilization produces a better range of motion (ROM) than the Kleinert regimen when place and hold are added. Sara Chevalley et al’s RCT investigating whether active mobilization is superior to passive mobilization with place and hold, after flexor tendon repair in the fingers, found no significant difference between the 2 groups for any of the outcome measurements, ROM, grip strength, key pinch, rupture frequency, Disabilities of the Arm, Shoulder and Hand score, ABILHAND questionnaire, and performance on the Purdue Pegboard test.
Check out these events:
-
58th Annual Meeting of Scoliosis Research Society - Seattle, US 6-9 September 2023
-
2023 AOA Annual Scientific Meeting: Rural surgery – build it and they will come
Melbourne Convention and Exhibition Centre, VIC - 12 Nov - 16 Nov 2023
-
The 67th Annual Congress of the Korean Orthopaedic Association - Incheon, Seoul, KR - 12-14 October 2023
Answer for the last month’s question:
The most common organisms responsible for the infection in shoulder arthroplasty are Cutibacterium acnes (formerly Propionibacterium acnes) (∼39%) and coagulase-negative Staphylococcus (∼29%)
Question of the month:
A patient with Pronator Syndrome presents with a positive Tinel sign in the proximal anterior forearm but no Tinel sign at the wrist and resists elbow flexion with forearm supination. He also has sensory disturbances over the distribution of the palmar cutaneous branch of the median nerve
Where is the level of compression?
a)compression at bicepital aponeurosis
b)compression at two heads of pronator teres
c)compression at FDS fibrous arch
Well, wait for our next issue to know the answer!
Have a marvelous May!