An update for the art of shouldering SHOULDERS!
Enjoy the updates on Shoulder with this issue of BWB
Bed in! (Bio-Sticky tack!)
Rotator cuff injuries can be life changing. Case in point, Kobe Bryant whose performance dipped because of it, while The Tiger Woods happened because he had to move away from baseball due to the same. It’s not so uncommon for your favourite athlete has to go on a long time off to recover.
Recovery rate is slow because of time needed for reliable tendon to bone healing before stress testing. Also, there is re-tear. Studies suggest it can 15% higher at 3 months, up to 16% at 6 months. Some suggest up to 40% in large tears. Where do we turn in these cases? Biologics - especially in large tears.
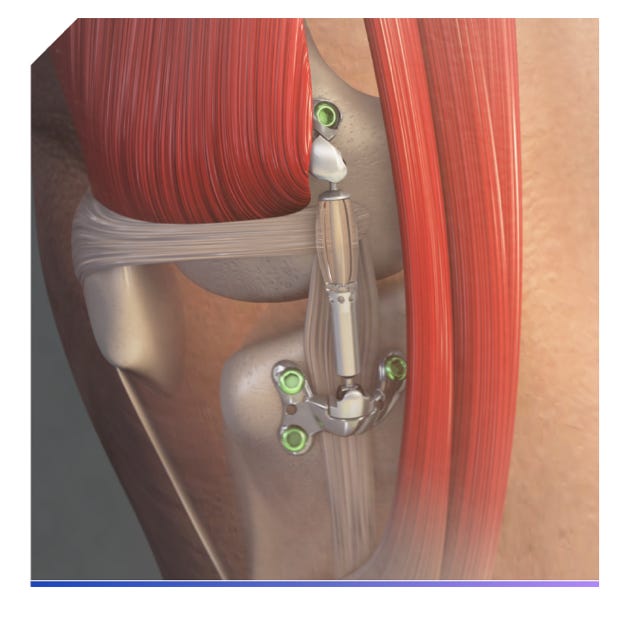
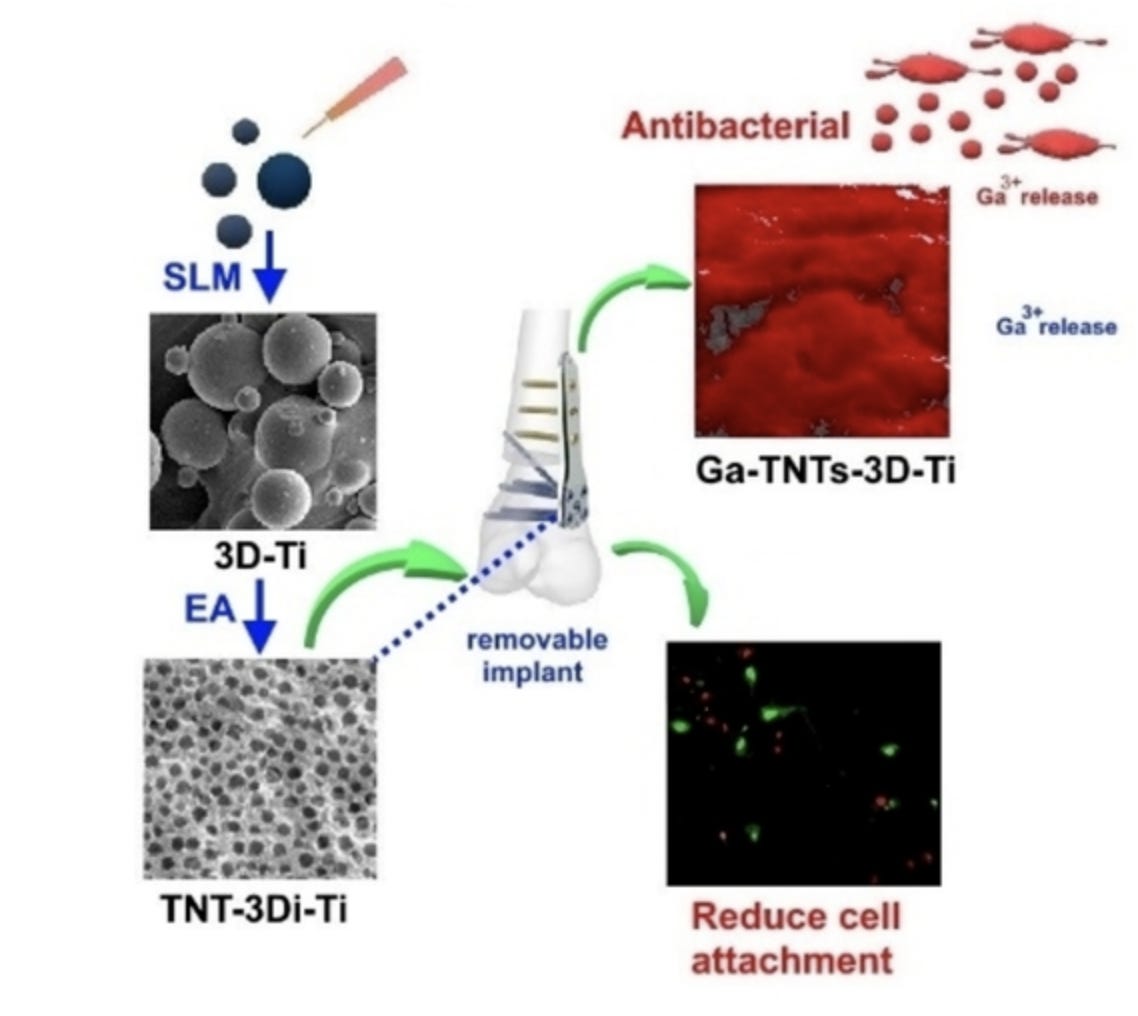
Sparta Biopharma (love the name!) have brought out a Scope compatible memory foam mattress to make a better bone repair interface. It is BioEnthesisTM , a biphasic allogenic, acellular, cancellous bone allograft that is placed inter-positionally between the decorticated humeral head and torn tendon(s) - thus helping us to manage massive tears. The biphasic composition promotes both osteointegration along with intact porous collagenous matrix for tendinous healing. It’s literally placing a sticky tack - Made of Human allograft and requires 15 minutes to rehydrate.
Animal studies at 12 weeks post op, show new bone formation and enthesis regeneration with Hi-Mag images show Sharpey fibres formation. As of now no clinical studies available to look at results. Check the detailed procedure here

From being a bail out option to becoming Gold Standard? - A tale of origin of Latarjet procedure - #FromTheHistory
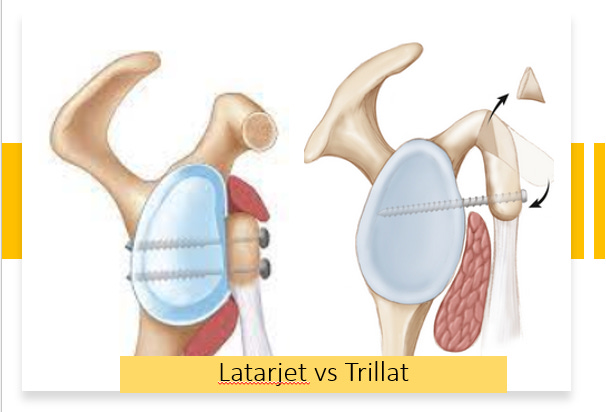
Latarjet procedure is almost a gold standard for anterior shoulder instability. With the definition of critical and subcritical bone loss coming down miraculously over years, the indications of this procedure is increasing. Let’s know some interesting stuff about early development of this procedure.
Lyon, which is the Mecca of Shoulder surgery, also happens to be the place where this procedure was developed. Albert Trillat, a pioneer of Orthopaedics was the first Orthopaedician at Lyon. He developed his own procedure for treating shoulder dislocations - the Trillat procedure where, Subtotal osteotomy of coracoid was done and the vertical arm of coracoid was shifted to glenoid, fixing it with a nail to the glenoid. Some of the unique features of this procedure are, the subscapularis is retracted and not split, there is a gap between the coracoid tip and glenoid which is filled by subscapularis, and sling effect of conjoint tendon is present. Between 1950 and 1953 Trillat performed 17 such surgeries. On a fine morning of 1953, Michael Latarjet, a general surgeon in Lyon, visited Trillat in his OR to learn his procedure. When he tried to reciprocate the same procedure on one of his patients, he accidentally fractured the coracoid. He then, as a bail out measure, transferred it to anterior glenoid by vertically splitting the subscap. Since the patient was doing well, he repeated the same in other patients as well. Ironically both published their techniques in the same edition of Lyon Chirurgical in 1954 - Trillat reporting outcomes of 17 patients and Latarjet - 4 patients. Over years, the Latarjet procedure underwent several modifications to incorporate the sling effect and attained the present form.
DAS is the new BOSS: #SurgicalPearl

We have been grinding old wine in a new bottle for a long time now. Bankart repair and Laterjet procedure are the two names, doing rounds in the instability world for the past 60 years. Remplissage by Wolf et al was one new technique that was described almost 2 decades back. In this backdrop, Dynamic Anterior Instability seems to be a new innovation in the field.
Described by Collin et al, it seems to be a great arthroscopic technique for limited glenoid bone loss.
-
From lateral viewing portal, glenoid neck is prepared at around 3 o'clock with a burr.
-
LHB is then tenotomized and then exteriorized and secured using whip stitch.
-
Split in the middle of the subscapularis using a switching stick, is made.
-
A hole at 3 o'clock from anterior to posterior within the neck of the glenoid is made.
-
The LHB tendon is then passed through the subscapularis split into the predrilled hole, to establish the “sling effect,” and fixed using a SwiveLock Tenodesis screw.
-
Bankart repair is then performed.
Check the video here
Acute type III ACJ dislocation: Conservative / Surgical?
Rockwood type III - do you operate or conserve? This debate has been going on for a long time now. Well let’s see the Riccardo Giai Via et al’s word on this. Their recent systematic review with Meta-Analysis included five studies with 73 and 110 patients treated with conservative and surgical approaches, respectively. Only the acromioclavicular distance was significantly reduced in the surgical group when compared with the conserved group. Constant score and coracoclavicular distances were similar between the two groups. So, conservative management is equally good as compared to surgical management in acute type-III ACJ dislocation.
Against the wave!
Is fibular strut graft really useful in proximal humerus fractures? 90 percent of us will be affirmative. But Qiuke Wang et al are negative for the its usefulness!. The fact that their study is one of the very few RCTs with 24 months follow-up makes them more credible.
80 patients were randomized. 39 were treated with fibular allograft and LCP whereaas the remaining were treated with only LCP. There was no change in functional outcomes, neck shaft angle or humeral head height between the two groups. Interesting right? Check out their paper in JBJS

Check out the events that line up:
-
13 July 2023 - 16 July 2023 - The American Orthopaedic Society for Sports Medicine (AOSSM) 2023 Annual Meeting - Washington DC , United States
-
08 June 2023 - 10 June 2023 The Practical Course in Orthopedics
Toulouse, France -
18 June 2023 - 21 June 2023 14th Biennial ISAKOS Congress 2023
Boston, United States
Answer for the last month question:
What are the clinical Guidelines for the Surgical Management of Chronic Lateral Ankle Instability according to the American Foot and Ankle Society?
Patients who continue to have symptoms of CLAI after 3 to 6 months of nonsurgical treatment and have indications of CLAI on physical and imaging examinations (stress radiography or MRI) are ideal for ATFL reconstruction.
Check this out for further read.
Question of the month:
What is the most common organism causing periprosthetic joint infection in shoulder arthroplasty?
-
Cutibacterium acnes
-
Coagulase-negative Staphylococcus
-
Staph. aureus
-
E. Coli
Wait for our next issue to know the answer.