"Men don't stumble, even over mountains!"
An update on managing some common complications as you brew with bones

Everyone deserves a second chance! - #NeoArmory
You should create one for yourself when life doesn’t give you a second chance.
Or Meshworks let 3D-print it for you...
Yes. Meshworks are a medical arm of the Alloyed group based in the UK. They have partnered with Orthosolutions, the well-known foot and ankle implant specialists. Now we have a patient-specific, 3D printed titanium truss for talar bone loss. A better way to put it is “talar bone loss specific implant” for fixation.
Design is by engineers using patients’ CT alongside the Surgeon who decides the bone cuts, real-time online in under 90 mins. Once the design and size are confirmed the order is shipped within 2 weeks. They come either as sphere or keystone with or without talar articulation, fixed with hind foot nails and additional screws with or without allografts
Bone ingrowth strengthens the construct and the truss helps in maintaining limb length. Some case reports show good follow-ups. Fusion rates seem as high as 85%. Complications like nonunion and infection can occur. Another issue is the cost which will take time to come down as titanium 3D printings become more common. Second chances are indeed priceless.

The Serendipity of electrocautery - #FromTheHistory:
The importance of eletrocautery cannot be overstated. It’s the go-to instrument for every surgeon in OR to manage and minimize bleed. But, do you guys know the interesting story behind its development?
Well, in the late 18th century, researchers were exploring various uses of current passed through the body. d’Arsonval showed that the current influenced body temperature, oxygen absorption, and carbon dioxide elimination. Franz Nagelschmidt discovered that patients with articular and circulatory ailments benefited from the application of electrical currents. He coined the term diathermy. Parisian physician, Joseph Rivere, while treating an insomniac patient with electricity produced by a generator noted that a spark arcing from an electrode coagulated an area of his skin. He subsequently used this arcing current to treat a carcinomatous ulcer on the hand of a patient.
This event has been cited as the first true use of electricity in surgery. Devices were then developed and improvised by many for this purpose. It was William T Bovie who developed the modern-day device with separate cutting and coagulating options. This device was first tried by the renowned neurosurgeon Dr. Harvey Cushing of Cushing’s disease to remove vascular myeloma.

Impaction Bone Grafting and Valgus osteotomy - #SurgicalPearl
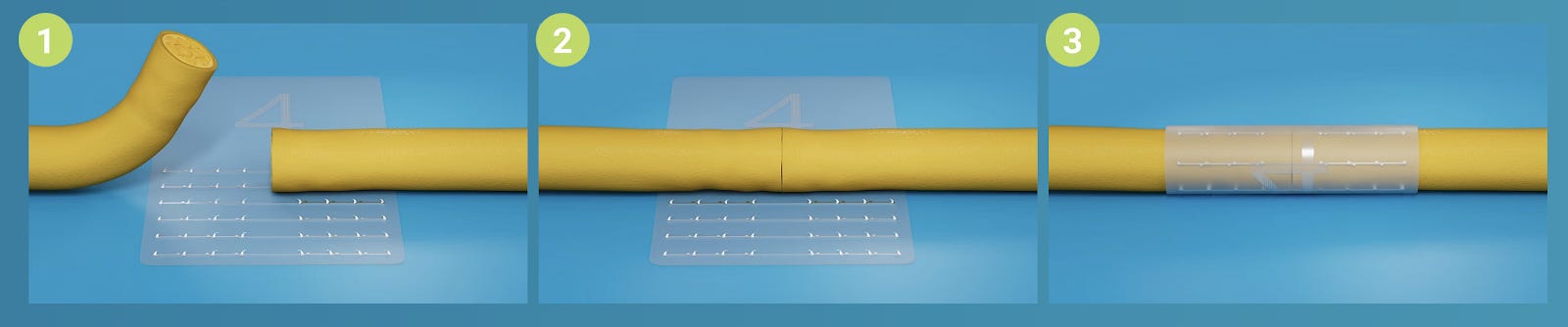
Pissed off due to a femur neck non-union in a young patient? Well, here is the hip salvage technique by Dheenadhayalan et al. This involves a routine valgus osteotomy and closed debridement of the non-union site using special curettes, followed by impaction bone grafting. The authors have reported a 95% success rate with this technique,


The morselized graft is delivered at the fracture site using these special impaction instruments. This is followed by reaming and reverse reaming slowly to further impact the grafts. Finally, a valgus osteotomy is done and fixation is completed with the appropriate sliding hip screw. We are known for brevity. Read the full article here.
Is DCO a cause of nonunion? - #MostCited
Hofman et al. analyzed the risk factors for non-union in diaphyseal fractures post-nailing. They found that the total number of surgeries before fracture consolidation was an independent predictor of non-union. This includes DCO (Damage Control Orthopaedics) procedures too. The number of operations performed in patients with long bone fractures should be kept as low as possible and the indication for and the timing of DCO treatment should be meticulously noted to minimize the risk of non-union development.
Answer to the last month's Question
Which among the following is a major predictor of no-show in a pediatric orthopedic clinic?
a. Insurance status
b. Waiting period
c. Clinic type
Answer: All of the above
Based on the study by Robaina et al. no-shows in pediatric orthopedic clinics depend on the payer type, duration between the scheduling and appointment date, and the specialty nature of the clinic.
Check out these hot events:
33rd Annual Congress of the International Society for Technology in Arthroplasty
World Orthopaedic Research Congress
Question of the Month:
Can the fixation of periprosthetic fractures of the hip and knee be delayed (>24 hours)?
Yes/No
What does a rigorous meta-analysis on the outcome of 3006 periprosthetic fracture fixations tell us? Hold your curiosity till we bring it to you in our August issue.
Have a jubilant July!