“Technology is indistinguishable from magic ” - Arthur C. Clarke
A sneak-peak into MSK Radiology 2.O as you brew with bones
Plan your Op. with JARVIS! - #NeoArmory
Remember Jarvis? Ironman’s augmented reality enabled supercomputer which can digitally dismantle things to study them. What if you can do the same for planning a complex fracture fixation??

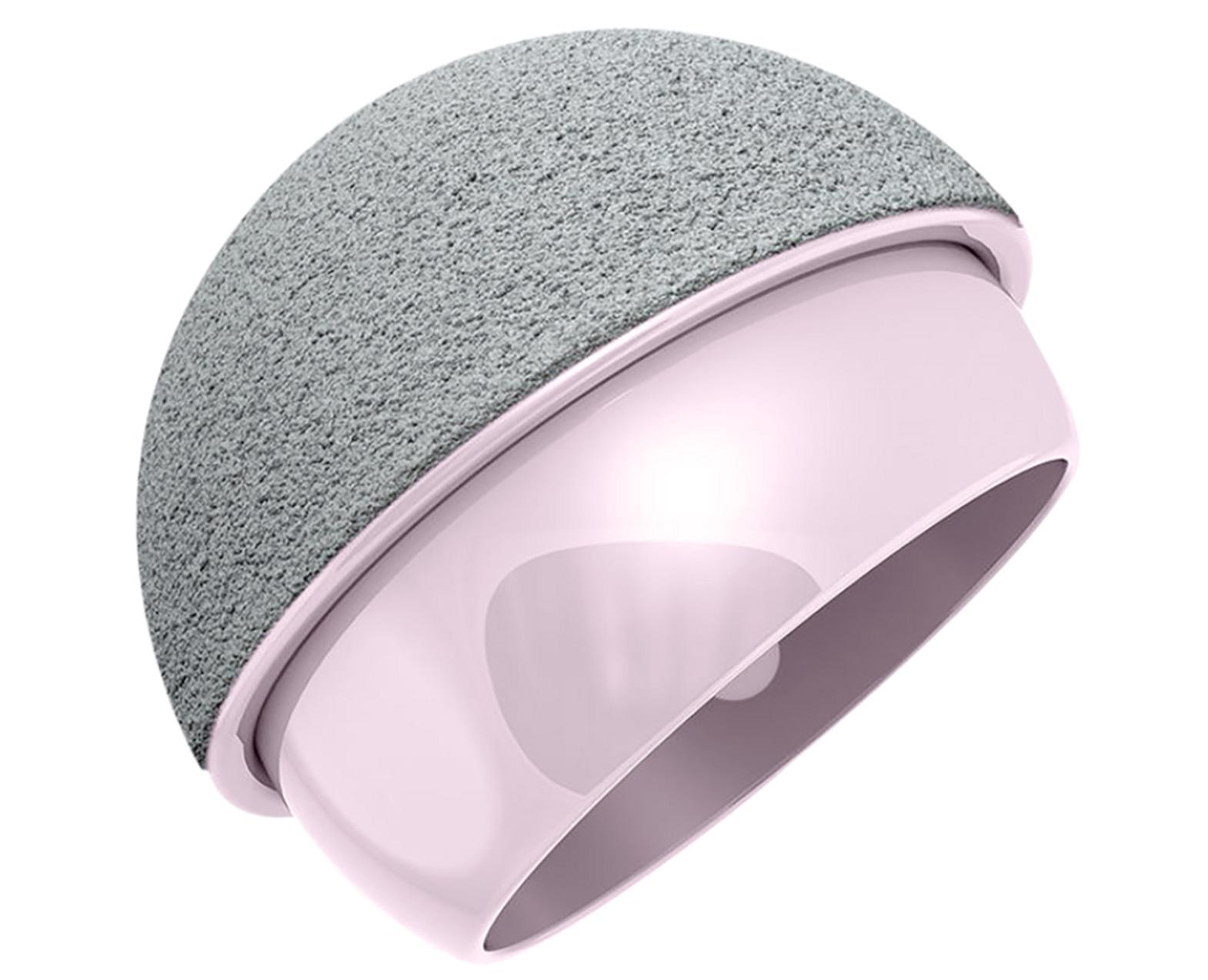
Introducing “SECTRA 3D Trauma”, from Sweden!
It uses input from a CT scan to give you a digital 3D model that can be used for pre-op planning. You can color code fracture fragments, move them around and reduce them, the ‘explode’ option moves the fragments away and they can be reconstructed one by one. An extensive library of implants from the major manufacturers can be used for templating. Also, contour the plates and measure the screw sizes. You can export the final plan to the 3D printer. It has its utility in spinal deformity correction and osteotomy as well
The benefits are for you to imagine.
Good reproducibility, better reduction accuracy, and improved operative efficacy have been noted in some studies. Cost is the only downside.
From binary stars to blood flow: The Japanese story of modern-day doppler scans – #FromTheHistory:
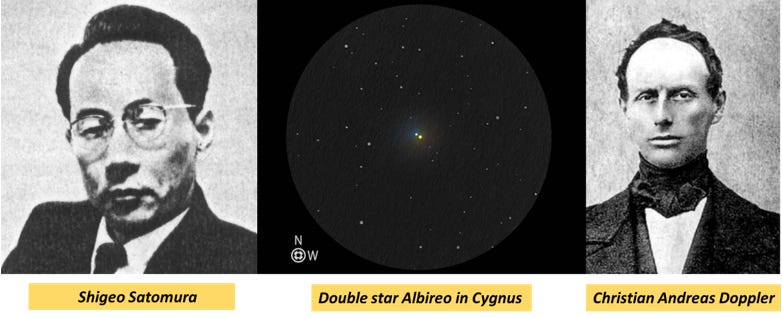
"On the colored light of the binary stars and some other stars of the heavens"
is the lecture that Christian Andreas Doppler delivered to the Royal Bohemian Society of Sciences explaining the logic behind the color of binary stars in 1842. Known as the Doppler effect – his principle that the observed frequency of a wave depends on the relative speed of the source and the observer became widely used in all fields from the theories of the universe to the military.
But not until 1956, that this principle started penetrating the medical field. Shigeo Satomura, a physicist from Japan was the first to use the doppler effect to analyze blood flow. He published his seminal work in 1956 titled ultrasonic doppler method for the inspection of cardiac functions. Shigeo Satomura was the heart of a multidisciplinary team of physicians joining the expertise of engineers in various research projects for the development of doppler technology. In recognition of his new interest in medicine and full dedication to developing engineering tools for medical applications, Satomura was awarded the degree of Doctor in Medical Sciences in 1960.
All with threads and needles: #SurgicalPearl:
Know about a simple 5-step scar-free outpatient US-guided carpal tunnel release popularised by the Mayo clinic.
· Using Ultrasound, the median nerve is localized in the wrist.
· Under local anesthesia, a modified Tuohy needle is passed under the carpal tunnel and above the median nerve by hydro dissection.
· The needle's tip is pushed above the exit point, and a cutting thread is passed through the needle.
· The Tuohy needle is then passed above the carpal ligament using the same entrance and exit needle holes as the first needle pass.
· That creates a complete loop around the ligament. The thread is pulled back and forth to cut the ligament.

Check out the original publication by Verena et al.
Almost no one is perfect! Alteast no knee is. Don’t treat your MRIs #MostCited
MRI abnormalities in asymptotic knees are not new. But, as the 3T scans are becoming a fashion these days, Laura et al report that 97% of asymptomatic knees had some abnormality in 3T MRIs that would tempt an arthroscopist to get the patient into OR.
Cartilage and bone marrow changes at the patellofemoral joint were seen in more than half the cases. 30% of knees had meniscal tears: horizontal (23%), complex (3%), vertical (2%), radial (2%), and bucket handle (1%).
The message is loud and clear. Unless you have a clinical diagnosis that necessitates an MRI validation don't do MRI.

Dr. CAD - #InTheTrials
Who checks the trauma x-rays first in the ER?
Well, the Emergency medicine clinicians. How long does it take for an expert Ortho or Radio opinion? - May be hours!

Lindsey et al. developed a computer-assisted detection (CAD) using a deep neural network to detect and localize fractures in radiographs. They emulated the expertise of 18 senior subspecialised orthopedic surgeons by annotating 135,409 radiographs to train the network. The CAD assistance improved the sensitivity by 10% and specificity by 6%, thereby reducing the misinterpretation rate by 47%.
Yeah, Dr. CAD will bail us out.
Check these cool events lining up!
-
8th International Musculoskeletal Ultra Sound Course - Athina, Greece
-
OTdigital 2022 – Congress for Digitalisation in Orthopaedics & Traumatology - Berlin, Germany
-
Wound Care, Tissue Repair and Regenerative Medicine 2022 - Dubai, United Arab Emirates
Answer for the last month’s question:
Second Opinions in Spine Surgery
Ferreira et al. made a systematic review on various aspects of the second opinion sought for spine surgery. Here are the facts from their systematic review:
-
Second opinions are initiated by patients, doctors, and payers.
-
Diagnostic agreement varied from 53-96%
-
Least diagnostic agreement: Cervical radiculopathy
-
Surgery agreement varied from 0-83%
-
Surgery most often considered unnecessary: Spinal fusion
Question of the month:
A picture to test Y’all.

What is the classical sign? Should we operate on this patient?
Wait for our next issue for the answer.
Have a blockbuster October ahead!