Hype - Heup - Hufte - Hop - Happy ????????????????
Hip it is! Enjoy the latest updates on hip in this issue.
Slithers and settles...
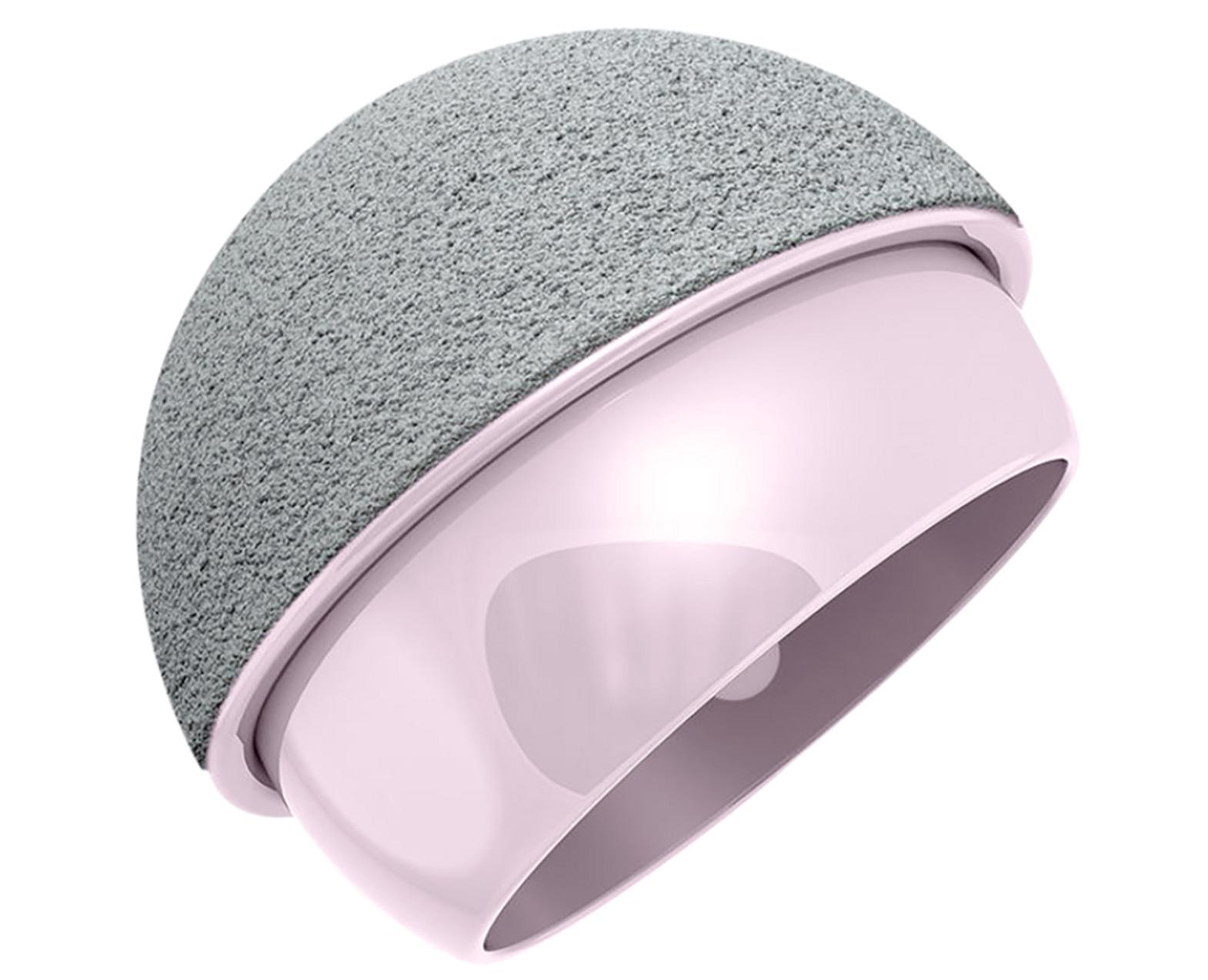
Placing a straight screw into a pelvic ring is difficult. You know why?.. well because it is…a ring. So why not think about a curved implant which can be inserted with a steerable guide wire predictably and stiffen up once inserted so that it can provide stable fixation while all this being done minimally invasive? Yes, That’s what CurvaFix brings to the table.
It is the first intramedullary implant to follow natural curvature of the pelvis, filling the bony canals, provides a greater force to failure and minimizes risk of pull out. It is touted to reduce the operating time to as less as 20 minutes and can bend up to 65mm radius of curvature. They have 4 equal length cables in the implant which can be locked at the end to provide rigidity.

Personally, the best part is the steerable guide seen in the video. A feasibility study done by the team using CT analysis shows the minimum radius of curvature is more than 65mm and the minimum (constriction point) diameter is 12+- 3mm. These implants come in 9.5mm outer diameter and varying lengths.
These are in early stages in development with a few promising case studies. I have high hopes as they aim solve one of the biggest issues in trauma surgery. Follow this space for any updates.

It slithers n settles
Who was on Sir John Charnley’s team? #FromTheHistory:
Well many were!
But Thackray’s were most notable.
When Charnley was at the Manchester Royal Infirmary, he had first asked Thackray’s to make instruments for him in 1947. His most notable collaboration with the firm was however, the total hip replacement. Thackray’s made the stainless steel stems, while Charnley made the sockets himself, turning them on a lathe in his workshop at home. In 1963, Thackray’s took over the socket production as well.
Teflon was used for socket production first. Eventually it was found that Teflon was not the ideal material for sockets. Charnley tested a high molecular weight polythene material, by implanting a sample in his own thigh. When there was no reaction, after six months he began to use it with patients.
He was however, worried about the long term results. So he did not let others to try it out untill his long term studies were encouraging. Even after five years, he allowed Thackray’s to sell only to those surgeons whom he had personally approved. In due course, anyone who had spent a minimum of two days learning the technique at Wrightington could buy his prosthesis. Charnley was collaborating with the Thackray’s until his death in 1982 to refine his total joint prosthesis.
They teamed up for a life time!
Thackray Medical Museum and the Thackray fellowship at Wrightington are a good tribute.

Lateral trochanteric wall reconstruction: #SurgicalPearl:
ZM Jafarullah et al divide lateral trochanteric wall fractures associated with peritrochanteric fractures into three types
-
Single fragment
-
With coronal split
-
Burst lateral wall fracture
Reconstruction is done according to the type of fracture using cerclage wires.
For eg: In type 3,
-
Aim was to buttress the lateral wall without disturbing the lateral soft tissue sleeve, to neutralize the abductor muscle pull and to prevent the intraoperative medialisation of the distal shaft.
-
This can be accomplished using two separate cerclage loops.
-
The proximal loop was passed around the abductors using cerclage wire passer and distally in the shaft using a drill hole.
-
Preliminary application of cerclage loops before nailing both proximally and distally helps to get the correct entry point and also helps to prevent the medialization of a shaft.
-
Once the nailing was done, both loops were fastened together to buttress the comminuted lateral wall.
Read the full technique here

Cemented vs cementless vs Hybrid hips - Which one lasts longer? #Most Cited:
Bloch et al. analysed a prospectively collected database with 10,112 THRs comprising of 1,699 cemented THRs, 5,782 hybrid THRs, and 2,631 cementless THRs with the revision at endpoint. 10-year survivorship was 97.0% in the cemented group, 97.6% in the hybrid group, and 97.9% in the cementless group.
The difference was not statistically significant.
Barring the spin, if we are to conclude objectively based on the results of the study, there is hardly any difference in failure rates between the three fixation methods.

Perfecting THAs - #Intrials:
As we are striving for perfection in THA, the Hip–spine relationship is the newly found culprit that might influence impingement, dislocation, and edge loading. Despite the safe zone orientation of the cup, abnormal hip–spine relationships have implications for implant position.
Robotic-assisted THA seems to solve this issue. Benjamin Domb et al at the American Hip Institute are into a Multicenter Trial involving Robotic Arm-assisted THA (Mako) 4.0 System. This version takes into account the Hip Spine Relationship and pelvic tilt in implant positioning. The study evaluates the hip angles executed by the Mako system intraoperatively using the postoperative 3D CT. Let’s hope that this would prove fruitful and take us a step closer to perfecting THAs.

Last month’s answer:
Well the wait is over guys.
According to Prada et al, 70% of Superficial SSIs settle with antibiotics in open fractures. Antibiotics seem to be the key.
Check these interesting events lining up:
-
2023 Arthroplasty Society of Australia Annual Scientific Meeting, Bowral, NSW - 18 May – 21 May 2023
-
9th Annecy Live Surgery Shoulder Advanced Course, Annecy, France - 8 June – 10 June 2023
-
Global Spine Congress 2023 Prague, Czech Republic - May 31 - June 3
Question of the month:
What are the indications according to AAOS guidelines to use Cement for stem fixation in Hip Arthroplasty?
Answer:
-
Abnormal proximal femoral morphology,
-
Conversion of failed hip fixation,
-
Inflammatory arthritis,
-
Osteoporotic bone.