Handy updates in Elbow, Wrist & Hand
Latest advancements in elbow, wrist, and hand treatments and care.
Unhinged - Unabridged! #NeoArmory:
Conquering longevity in Total Elbow Arthroplasty still seems out of reach and innovation seems to have reached a plateau. Hinge wear, stem pull-out, stress shielding, etc., keep making a mark in the ODEP rating.
Trying to solve all problems at once is ARRCH ORTHOPAEDICS’s style. Stem pullout? Intramedullary screw-in prosthesis with cross-locking screws may be the answer. Hinge wear? Let’s make is semi-constrained. Snap fit like Ikea. Tired of stress shielding? Reonstructed ligaments keep the bone occupied.

One of their proprietary techs includes the ‘Cylindrical Ligament Retention Device’ (also an excellent photographer) which fits into the prosthesis for mediolateral stability. Oh also, has your Hinge worn out? Just go in and replace the poly. Just like minor service for your car.
Please mind, that all these are theorized and extensively tested mechanically - yet to see any clinical studies and follow-up studies. Just have a look at their website. Extensive research and reasoning for everything from spool nuts to washer design.
After reading through their op-tech - only to realize there are another 3 PDFs to go through
The power of keen observation: #FromTheHistory
One can state, without exaggeration, that the observation of and the search for similarities and differences are the basis of all human knowledge - Alfred Nobel
Believe me! Once upon a time, distal radius fractures were considered wrist dislocations.
“This fracture takes place at about an inch and a half above the carpal extremity of the radius and exhibits the following appearances” wrote Dr Abraham Colles in his classic paper published in 1814, on extra-articular distal radius fracture, now called famously the Colles’ fracture. In 1760, Claude Pouteau, a French surgeon described these fractures and their characteristic angulations much before Colles’.
“but we shall concern ourselves principally with fractures that occur following falls, where the hand appears to have made the greatest efforts to stave off danger. These fractures are most often taken for sprains, for incomplete luxations…”
Claude Pouteau
Though these men described the same pathology 54 years apart they both deserve the credit given the times they lived. They were from different regions of the world and were poorly connected technologically. They dared to describe this fracture with much conviction, from their powers of observation, in days much before the discovery of x-rays. They not only described these fractures but also, described ways and means to reduce and treat them.

Pry & Leverage - #SurgicalPearl
Closed reduction and pinning for Paediatric Supracondylar humerus fractures is one of the more satisfying and quick procedures that we would like to do. Though we hate the open reduction of such fractures, sometimes the fracture patterns force us to open. Several techniques have been proposed to aid in the closed reduction of difficult fractures.
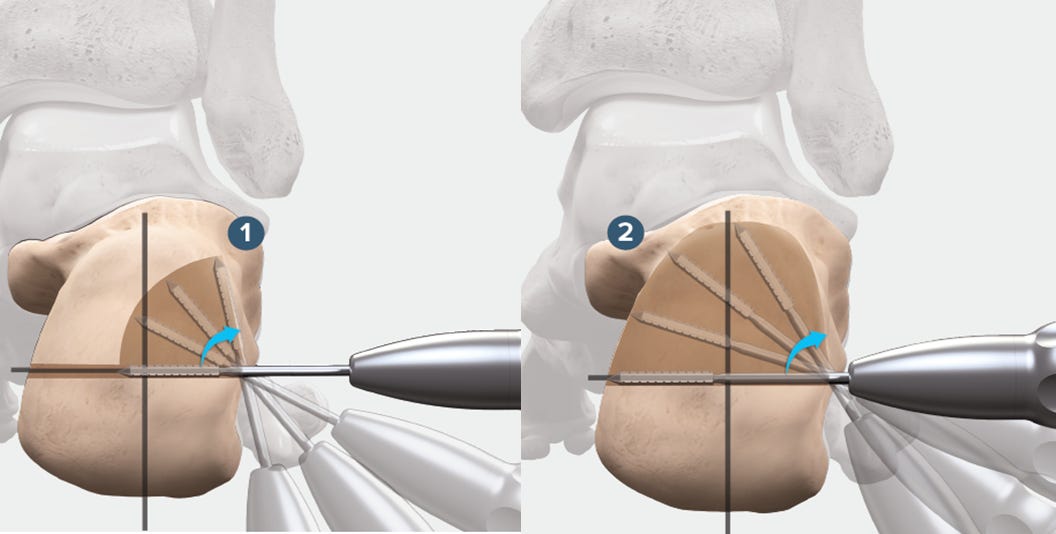
Prying and leveraging is one such new technique by Xiao et al. in Gartland type III and IV fractures.
Sometimes soft tissue between the fracture ends makes the fracture irreducible. In such instances prying is helpful. The blunt end of a 2.5 mm k wire is used to pry along the medial and lateral ridges of the distal humerus to relieve the soft tissues from proximal to distal. This relieves the interspersed soft tissues and aids in fracture reduction.
In highly unstable type IV fractures, leverage can be used to hold reduction temporarily until K wires are applied. Here, again a 2.5 mm wire’s blunt edge is passed across the fracture site from posterior to anterior and it is leveraged to hold reduction.
Learn more about these simple yet effective tips here

WALANT - for the valiant #MostCited:
The Wide-Awake Local Anesthesia No Tourniquet (WALANT) method is in the trending stories of hand surgery communities. Conservatives argue that it may increase the risk of infection. Rellen et al. in their study of 526 patients, compared the infection rates and complications in Carpal Tunnel release and trigger finger release surgeries using WALANT and monitored anaesthetic care.
To their surprise, in patients undergoing carpal tunnel release, there were no infections with WALANT and 6 infections (2.2%) with MAC. In patients undergoing trigger finger release, there were no infections in either group. There were similar rates of complications noted in both groups.
Having the patient awake during surgery makes you a cool and safe surgeon.
Collagenase Vs Needle Fasciotomy #InTrials:
Many times a simple procedure (NB: Nothing is simple in surgery) gets overshadowed by a new product getting aggressively promoted. One such procedure was needle fasciotomy. Martin et al, however, highlight the effectiveness of needle fasciotomy in their comprehensive 5-year study in terms of clinical outcomes and patient-reported experiences. 156 patients were randomly assigned to receive either NF or collagenase Clostridium histolyticum treatment. No significant differences were found between the two treatments concerning passive joint extension, contracture reduction, range of motion, or patient-reported outcomes.
Many a time, simple treatment is all that is required!

Cool Events to check out:
-
International Society for Computer-Assisted Orthopaedic Surgery (CAOS) Congress 19-22 June 2024 - Groningen, Netherlands
-
The 35th International Congress of International Society for Technology in Arthroplasty (ISTA) 28 -31 August 2024 - Nashville, USA
-
59th SRS Annual Meeting of Scoliosis Research Society (SRS) 10 - 14 September 2024 - Barcelona, Spain
Answer to last month’s question:
What is considered a significant glenoid bone for inferior outcomes in arthroscopic Bankart repair?
-
21%
-
20%
-
17.5%
-
13.5%
Answer: According to Tokish et al, a bone loss of 13.5% should be considered critical as a loss of more than 13.5% resulted in a significant decrease in WOSI scores.
Question of the month:
In conservative management of scaphoid fractures, which is true?