When LESS IS MORE
Brew with the exclusive curation of next-gen minimally invasive Orthopaedics
This thing gives us quality sleep!
“What keeps an average Joe awake all night? “I asked my 3-year-old.
“Monster in the closet...” she replied, with an audible gasp.
“What keeps you awake?” questioned back my curious kid
Well, Wound breakdown, neurovascular compromise, infection, and exposed implants were the ones that stalled my mind.
What if all these come in a single compact package??
*Drum roll* *curtains up*
TA-DA… *a calcaneum gingerly walks to the stage and bows*
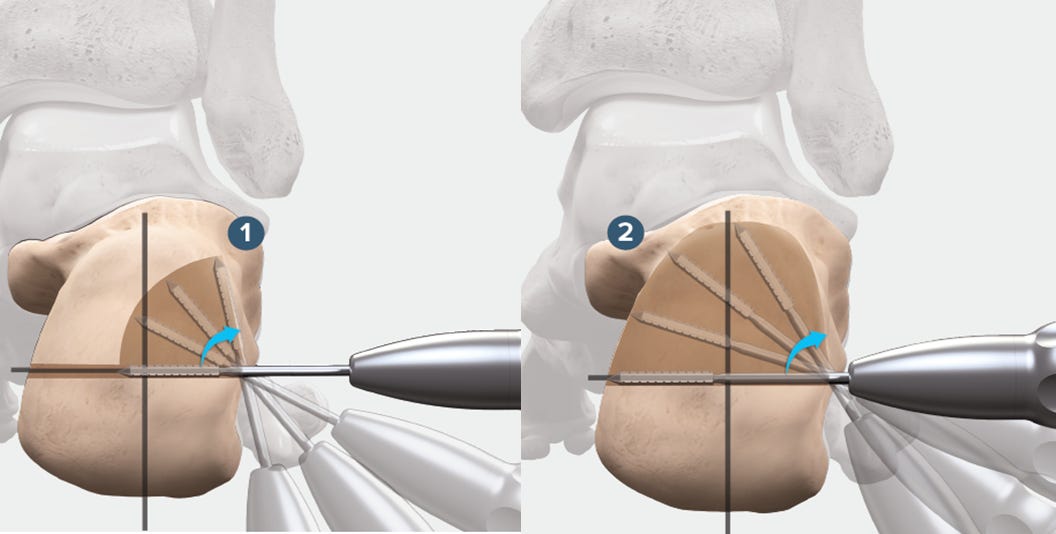
Yes, we all know the calcaneus carries an astounding number for the wound complications leading to infection, etc. And it’s not uncommon that we face a dilemma if we can get away without doing an osteotomy when it is actually needed.
As always with necessity, comes invention.
Yep, you guessed it, our good old friend MIS with the ever so fancy new name MIMCO - Minimally invasive medialising calcaneal osteotomy. Excellent techniques are available with Shannon Burrs – end and side cutting burrs. And when paired with low speed, high torque, pencil grip setup everyone is an artist during calcaneal osteotomy.
This is no slouch when you compare it with the traditional number. Check out the study by Kendal et al on MIMCO.

The person of this month to inspire you guys is none other than the man who actually showed the world “Less is more” in surgery - the man who coined the phrase “Minimally Invasive Surgery” - Prof. Parviz Kambin.
Born in Iran, Prof. Kambin shifted to the US for post-graduation. He completed his academic training in New Jersey Orthopaedic hospital. In his decorated carrier Prof. Kambin has to his credit International lectures, textbooks, research publications, literary publications, patents, and whatnot.
When the world was still perplexed about the complex and intricate anatomy of the spine, Prof. Kambin showed how Minimally Invasive Surgery is possible in the spine. His work brought about a shift in the way we treat spine pathologies, inspiring thousands of young surgeons into minimally invasive spine surgery

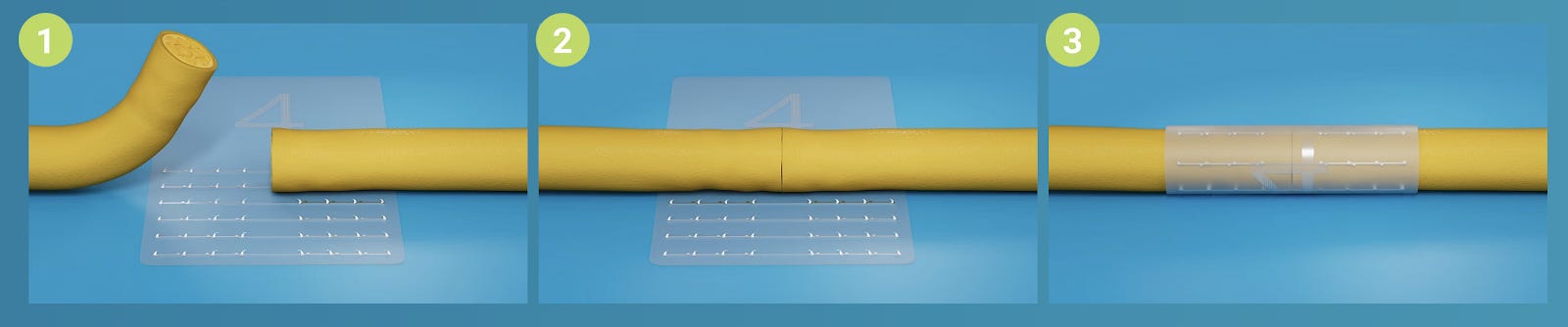
MIPPO Posterior plating for humerus shaft - surgical pearl
For those who are annoyed with the blood-filled surgical field in the posterior plating of the humerus shaft, Balam et al have shown us an elegant way to slide the plate and come out cool.

-
Make a 3 cm incision over the spiral groove
-
Identify and protect the radial nerve
-
Slide the plate and complete bridge plating
See, life is simple. No more war between cautery and the vessels
His and three other studies on minimally invasive posterior plating have shown excellent results. Check them out.
Is it worth it?
With all the whims and fancies of the Minimally Invasive Fusions going around, JL Heemskerk et al in their meta-analysis analyzed the clinical outcome of single-level OPEN Vs MI TLIF surgeries.
They noted that the long-term outcomes of both treatments are comparable. Both techniques (MI & OPEN) were successful in improving QoL, function, and pain for patients with single-level degenerative lumbar disease and the choice of the approach lies at the discretion of the surgeon.
The main advantage of MI-TLIF seems to be, however, peri-operative and directly postoperative.

Can we do it on one side only?
Generally, fusion supplemented with bilateral pedicle screw fixation (PSF) is the widely accepted method of stabilization. Bilateral fixation has its shortcomings in the form of adjacent lumbar segment degeneration, implant-related osteoporosis, longer surgical time, greater blood loss, and greater cost.
A relatively less rigid fixation in the form of unilateral fixation, described by Goel et al, could reduce the stress shielding and adjacent intervertebral disk degeneration caused by bilateral pedicle screw fixation.
Biomechanical studies also support this concept.
Unilateral fixation following fusion has been shown to give results on par with bilateral pedicle screw fixation in clinical studies.
Mind you, Cage migration has however been reported with unilateral fixation. And it’s not suitable for long-segment fixation as shown by S Muthu et al

Check the cool events lining up
- Here we come Goa! - IOACON 2021
- Onco lovers ???? Free online 3-day MSK oncology course
- Hybrid Eurospine 2021 conference - Vienna
Well, guys wait is over. Answer to the last month’s question is here
Fresh Vs stored blood:
Blood for transfusion is stored for up to 42 days. Most of the blood banks follow the first in first out policy so that the shelf period of the collected blood is shortened.
Older blood develops lesions and accumulates potentially injurious substances.
Wang et al. in their meta-analysis of 21 studies assessed the safety of transfused “old” versus “new” blood. Most of the studies included in the analysis considered the blood is old if it is stored for more than 2-3 weeks. Usage of such old blood increased the odds of death due to the transfusion by 16%.
What is the effect of lead aprons on your posture? Wait for our next issue on the first Sunday of October????????
Remember? Fresh is good - Always!
Start your month fresh!
Happy September????